TechMagic Academy
TechMagic AcademyAgentic AI for Healthcare Products: How to Move from Pilot Purgatory to Production
Last updated:9 June 2026


Gartner expects over 40% of agentic AI projects to be canceled by the end of 2027. Across the healthcare industry, the gap is just as stark, with only 21% of organizations reporting mature governance for agentic AI, even as 74% expect to use AI agents by 2027. Production lags far behind.
Healthcare products and agentic AI look like a natural fit on paper. You can demo an agentic feature in a single sprint, and it will impress the room. Six months later, though, it may still be sitting behind a flag, nowhere near real patient data.
The pilot does not fail loudly; it just never ships. And most of the time, the model itself is fine. The main reason for the failure is the product decisions around it.
In our new article on agentic AI for healthcare products, we cover why these pilots stall, what makes a medical product different from general enterprise AI, what production-ready actually looks like, and a phased roadmap to get there.
Key takeaways
- Most pilots stall for product reasons. The cause is architecture, and the model is rarely the problem.
- Three root causes repeat: incomplete context, undefined scope, and absent governance. Deloitte found that only 21% of organizations have a mature governance model for agentic AI.
- Healthcare adds constraints that enterprise AI avoids: Software as a Medical Device (SaMD) risk, protected health information (PHI) exposure, electronic health records (EHR) integration, and liability for autonomous action.
- Production-ready means five things: complete context, scoped autonomy with rollback, an auditable decision trail, tested edge cases, and real governance.
- The teams that ship start the same way. They find the context gap first, then scope one workflow and expand.
Why Do Most Agentic AI Pilots for Healthcare Products Fail to Reach Production?
Most pilots stall before they ever reach a patient, and the cause is almost always architectural. The product decisions get made before anyone writes a line of agent code, and then the model takes the blame for what was really a design gap. Gartner and Deloitte trace the failures to the same short list of reasons agentic AI adoption stalls short of production:
- Incomplete context. The agent reasons over a slice of the data and misses the rest of the chart.
- Undefined scope. The agent is asked to do everything, so it can be trusted with nothing.
- Absent governance. Nothing records what the agent did, so no auditor will sign off.
Each one is a product problem rather than a model problem, which is why a stronger model rarely rescues a stalled pilot. As a product leader, these are your calls to make: the data architecture, the agent scope, and the human oversight that sits on top.
You cannot prompt your way out of an architecture problem
Teams use different names for it. You might hear agentic AI for MedTech products, healthcare AI, or simply AI agents in healthcare. Whatever the label, the production problem underneath stays the same.
The cost of a stalled pilot is higher than a missed sprint. Healthcare organizations back these features to improve patient outcomes, widen patient access, lift patient engagement, and deliver more personalized care. When it never ships, none of that arrives, and the healthcare providers and healthcare leaders who were promised it quietly stop trusting the next pitch.
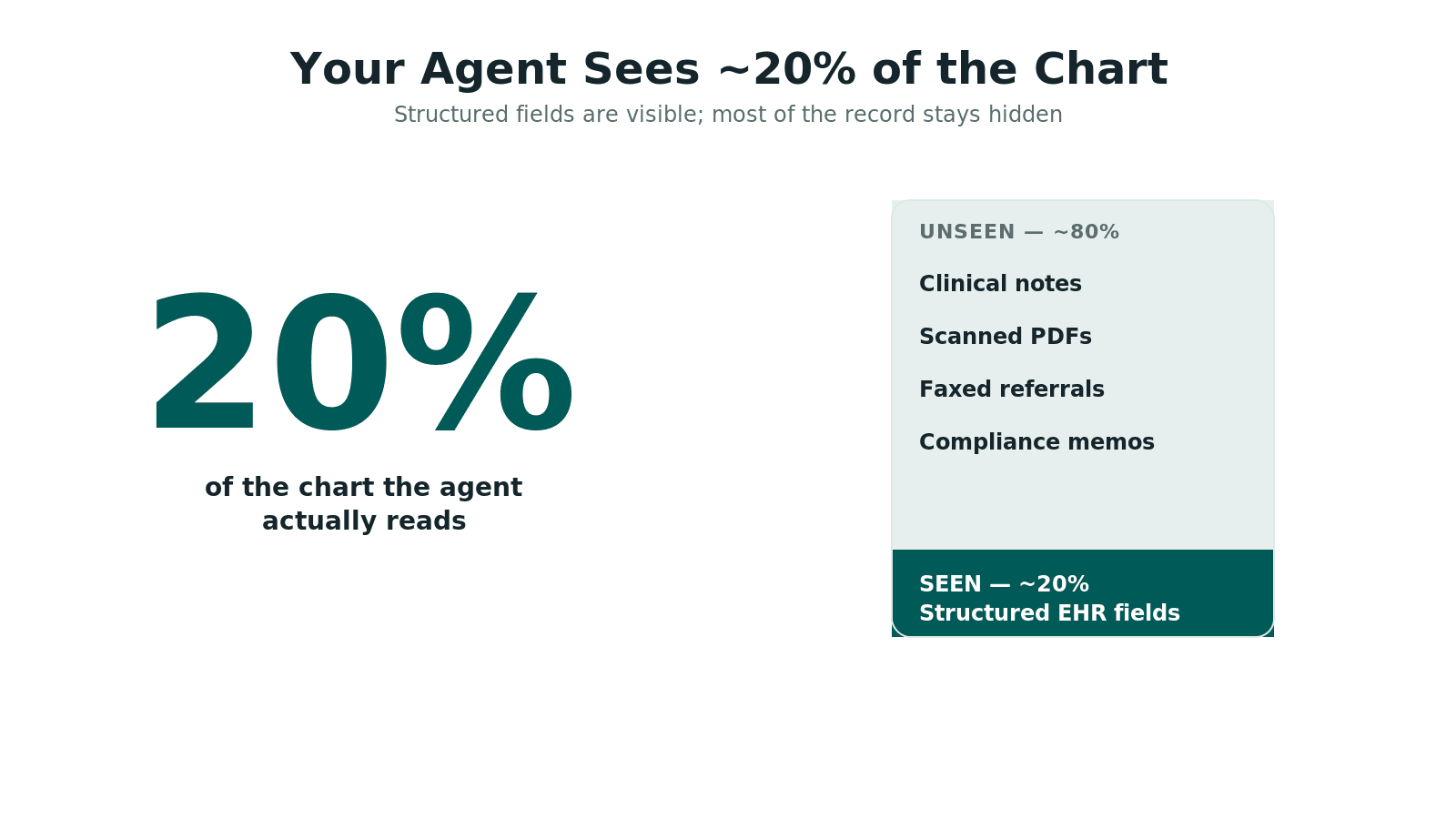
The context gap: why your agent is operating on 20% of your data
The context gap is the most common reason agentic AI for healthcare products stalls, because your agent can only reason over the data it can reach. In many pilots, that is roughly 20% of what exists. It sees the structured fields in electronic health records, but it misses the clinical notes, the scanned PDFs, the faxed referrals, and the compliance memos where the rest of the patient history lives.
When an agent cannot see that faxed referral, it ends up working from a partial chart. It might still produce a confident answer, and a clinician will catch the problem right away, because the agent never had the complex medical data that mattered. Closing the gap means integrating data from structured and unstructured sources before you scale, and Retrieval Augmented Generation (RAG) helps by pulling the right patient records and medical images into each step.
Nobody sets out to ship on 20% of the chart. It just creeps in, one shortcut at a time.
Scope creep in AI pilots: why "build everything" kills production
Scope creep is the quiet killer here. An agent asked to handle every case has to be tested on every case, and that testing never ends. A pilot that tries to automate intake, scheduling, prior authorization, and clinical documentation all at once has no clear bar for "done," and no safe place to start.
Narrow scope is the better bet: pick one workflow with measurable value, define what the agent may and may not do, and ship it. You can always expand later. Teams that try to build everything tend to ship nothing, because complex tasks multiply the testing, the compliance review, and the failure modes.
Governance theater vs. real oversight: what auditors and regulators expect
Governance theater looks like oversight, but it cannot answer the questions an auditor actually asks. Real oversight is concrete: defined decision boundaries, real-time monitoring, and an audit trail that captures every agent action. Deloitte's 2026 State of AI in the Enterprise survey makes the gap clear, with only 21% of organizations reporting a mature governance model for agentic AI, which means roughly 80% are scaling faster than their controls.
Auditors and regulators do not want a policy PDF. They want evidence: which decisions the agent made alone, which needed human approval, and what data each decision used. If your product cannot show that record on demand, the governance is theater, and the pilot will not clear a compliance review.
Roughly 80% of organizations are scaling agentic AI faster than their controls.
We help healthcare teams find the gap and close it

What Makes Agentic AI for Medical Products Different From General Enterprise AI?
Four healthcare-specific constraints set it apart, and they shape your architecture long before you tune anything for performance. When a retail or FinTech agent slips, you get a refund or a support ticket; when a clinical agent slips, it can affect patient safety. That raises the bar for scope, oversight, and evidence.
A wrong refund is an annoyance. A wrong clinical action is a safety event
This is also why the old Artificial Intelligence playbook does not quite carry over. Unlike traditional AI, an agentic feature does not hand you one output you can eyeball and approve. Traditional AI systems and traditional AI models answer a single question, and generative AI mainly produces text.
Agentic AI systems are different, because they plan and act across multiple steps. They build on the same AI algorithms in healthcare you already use, from Machine Learning to Large Language Models, but that autonomy multiplies what can break in production. We are not redefining the category here, just flagging why production gets harder.
Built to act inside clinical workflows, agentic AI has to earn its place like any other AI systems do. The same is true of AI-driven systems across healthcare technology: they only help if they fit real healthcare contexts. And most health care decisions carry real stakes.
The workflows vary by product. An agent might support clinicians with diagnostic support, flag cases for early identification, enable timely interventions, help draft treatment plans, or tailor more personalized patient care. Agents support that work, but they do not replace the human relationship that sits at the center of compassionate care.
The point is how each constraint changes a product decision. Where do you put the human checkpoints, how much autonomy do you grant, and what does your audit trail need to hold?
FDA SaMD risk: when does your agentic feature become a regulated device?
An agentic feature can become a regulated device once it influences a clinical decision. Clinical influence is the trigger, while administrative tasks usually stay clear. Under Software as a Medical Device (SaMD) rules, an agent that recommends a diagnosis may fall under the Food and Drug Administration (FDA), and so might one that suggests a treatment plan, while an agent that only drafts administrative documentation usually does not.
This is a scoping decision, and you should make it early, alongside your legal and regulatory teams. Watch your roadmap closely, because a feature can drift from scheduling toward diagnostic support, or even into clinical decision making, and cross a regulatory line without anyone noticing. Decide early, revisit the classification as the agent grows, and get a regulatory opinion whenever you are unsure.
PHI exposure in multi-step agentic workflows: architectural safeguards
Multi-step workflows raise PHI exposure because every step, tool call, and log is another place patient data can leak. A single prompt is simple to reason about. A full agent is more involved: it reads a record, calls an external service, writes a note, stores intermediate state, and each action is another place data security can fail.
Safeguards address this directly. Give each step the least PHI it needs, mask or tokenize patient data before it leaves your boundary, and keep audit logs that record access without copying sensitive fields into plain text. Patient privacy is a design constraint that applies to every step along the way.
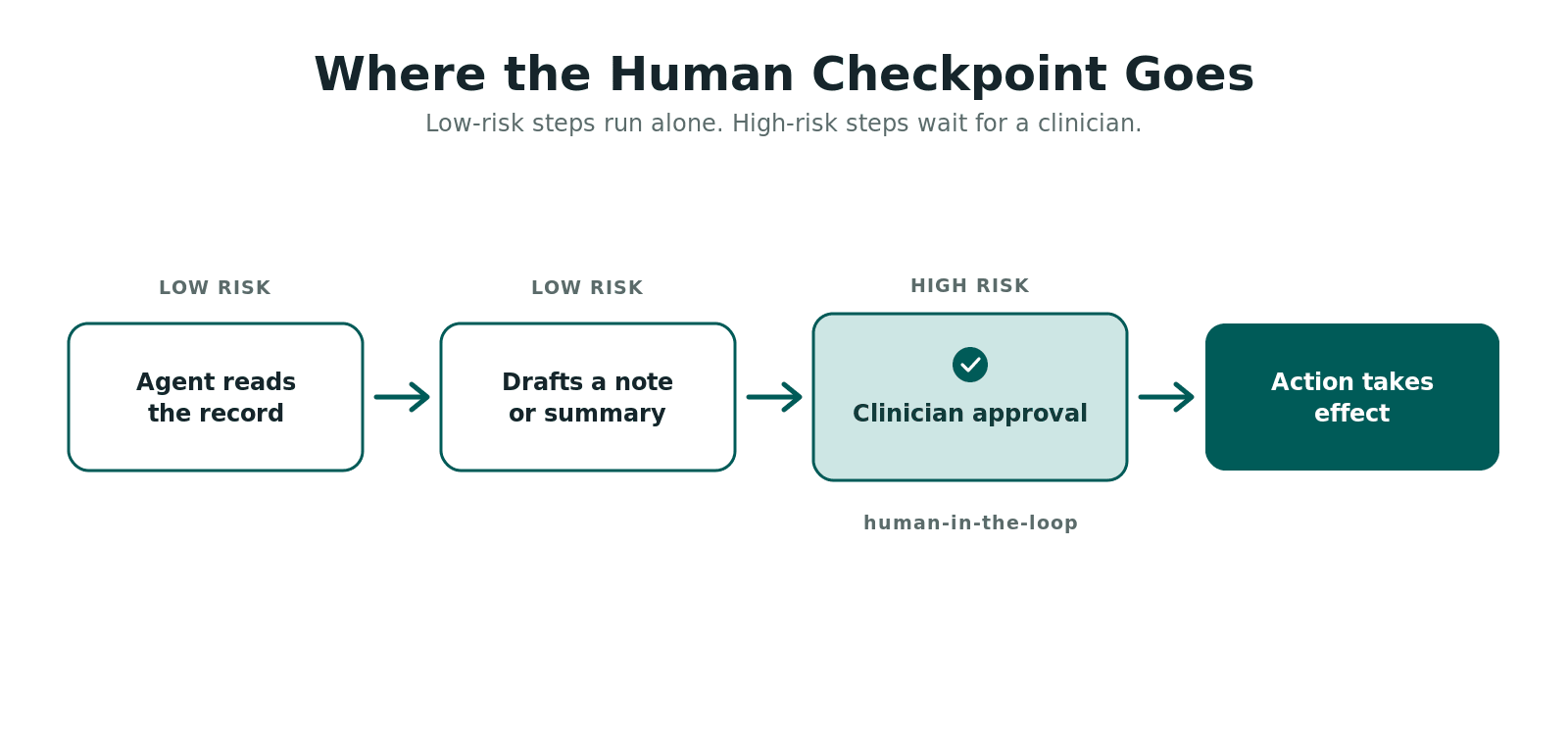
Human-in-the-loop design: where to put the checkpoints in a clinical product
Human-in-the-loop design comes down to risk: you decide what an agent does alone and what a clinician has to approve. Low-risk steps, like summarizing a note, can run with minimal human input, while high-risk steps need review first, and anything touching direct patient care belongs there.
The skill is placement: put checkpoints where they add safety without making the product useless. Too few checkpoints carry real risk, and too many drive clinicians away. Map each step to its risk, and reserve mandatory review for the moments where human expertise genuinely changes the outcome.
What Does Production-Ready Agentic AI Look Like in a Healthcare Product?
Production-ready has a clear definition. The agent works on a complete context, has a defined scope with rollback, and produces an auditable decision trail. It has been tested against adversarial clinical edge cases, and it runs under a governance model that satisfies both internal stakeholders and external auditors.
A pilot proves an idea can work once. Production proves it works safely, repeatedly, and under review. The gap between the two is concrete and shows up across five dimensions, which the table below lays out, contrasting what a pilot tolerates with what production requires.
HIPAA-compliant portal for secure medical data records and exchange

Data architecture: connecting structured and unstructured clinical data
Production data architecture connects structured and unstructured clinical data, so the agent reasons over the full chart instead of a fragment. You join electronic health records with the clinical notes, faxed referrals, and scanned documents that together hold most of the patient's medical histories your agent needs.
In practice, teams add a retrieval layer, and Retrieval Augmented Generation is the common choice for bringing the right patient history and real-time data into each step. Clean inputs matter just as much, so good data analysis comes first, and if the agent cannot analyze data that is current, even strong reasoning falls apart. Aim for one reliable source for the agent to query, because patient outcomes depend on its accuracy.
Testing for production: clinical edge cases your pilot probably missed
Production testing means hard cases. You run the agent against adversarial clinical edge cases that a happy-path demo skips. Clean records hide the problems, but real healthcare environments are messier, full of conflicting medication lists, ambiguous notes, and incomplete intake forms.
Build a test set from real edge cases and known failure modes, then watch how the agent behaves under pressure when context is missing or data conflicts. The goal is not perfection but predictable behavior: an uncertain agent should escalate to a human rather than guess. That one habit separates a tool that supports clinicians from one that quietly adds risk.
What an auditable agentic AI audit trail looks like
An auditable trail records each decision: what the agent did, what data it used, and whether a human approved it. This is the evidence auditors and regulators ask for, and it is the line between real oversight and theater.
A useful trail captures the input context, the chosen action, the tools the agent called, the human approval status, and the final outcome, all with timestamps and with raw PHI kept out of plain text. Build it from day one, and it doubles as your debugging log. Add it later, and it becomes an expensive retrofit, which is why pilots stall when a compliance review arrives.
How Do You Build a Product Roadmap That Moves Agentic AI From Pilot to Production?
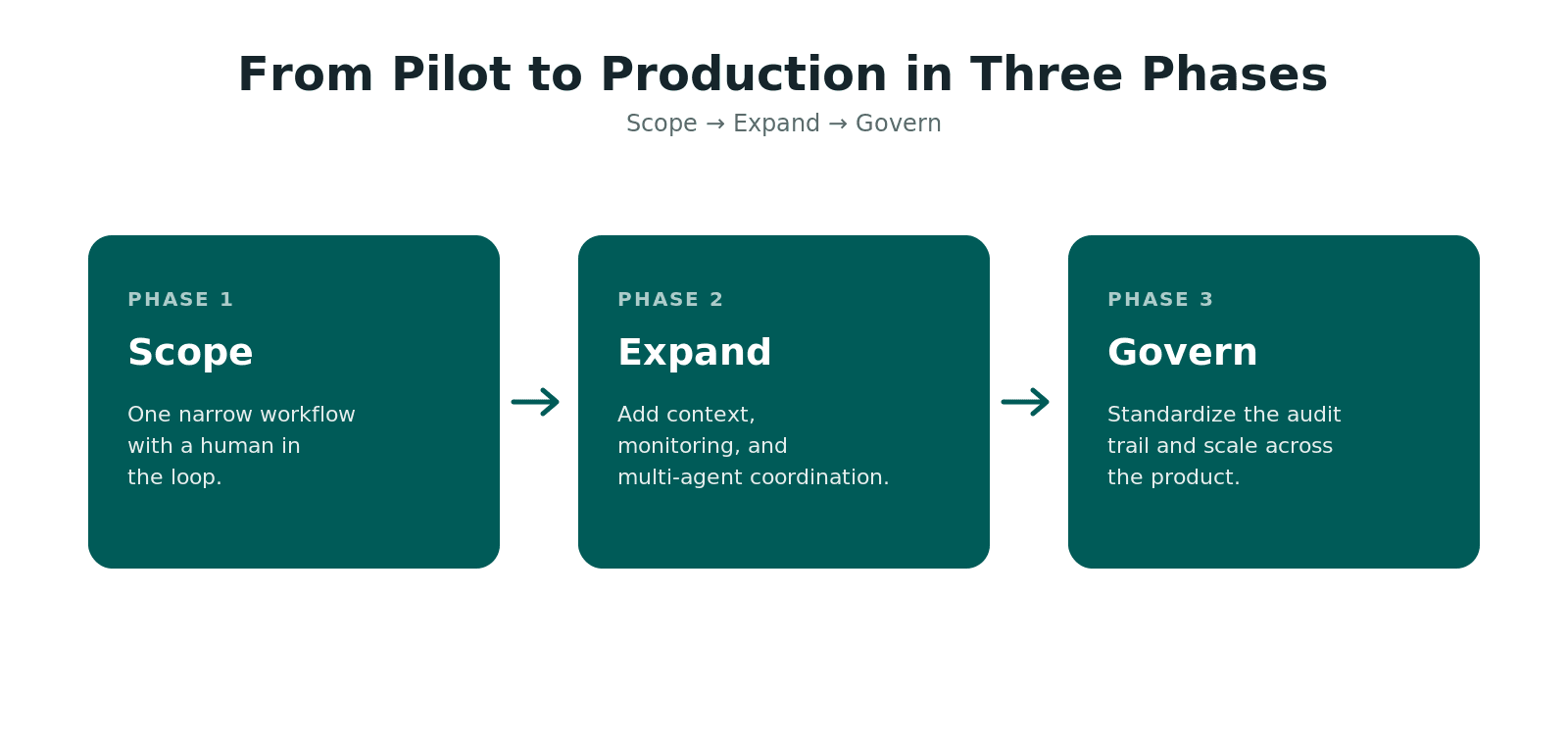
In general, we build the roadmap in three phases, starting with one narrow workflow and expanding context, coordination, and governance from there. The shape is simple:
Scope → Expand → Govern
From our experience, the teams reaching production in 2026 share one habit: they find their context gap first, before they build any architecture.
A few cautions apply throughout. Implementing agentic AI is not a seamless integration you switch on, and the applications of agentic AI in healthcare vary widely, from single agents to multi-agent systems. Each phase also raises ethical concerns and ethical considerations, like bias and consent, along with the compliance risks of autonomous action, so plan governance and resource allocation alongside features.
Below is a phased approach for healthcare product teams, with the build, buy, or integrate decision called out at each step.
Phase one: scoping your first production-grade agentic workflow
Phase one is a single workflow with a narrow scope and a human in the loop. Good candidates are documentation, prior authorization, and patient intake, because they carry clear value and lower clinical risk than direct diagnosis. Define what the agent may do, where a clinician approves, and how you roll back.
On the build, buy, or integrate call: for a first workflow, integrating an existing agent framework is usually faster than building from scratch. You want to validate the workflow and close the context gap, and maintaining a platform can wait. Reducing administrative burden on a single task is a strong first win.
Phase two: expanding context and adding multi-agent coordination
Phase two expands the agent's data context and adds monitoring, feedback loops, and multi-agent coordination, where it helps. You connect the unstructured sources you deferred in Phase one and watch how the agent handles a wider range of cases. This is also where you add the real-time monitoring that your governance model needs.
Multi-agent systems belong in this phase, once a single workflow is stable. Then specialized AI agents can hand off to each other, with one agent drafting clinical documentation and another checking it. On build, buy, or integrate: treat monitoring and orchestration as shared infrastructure, since every later workflow will reuse it.
Phase three: governance, monitoring, and scaling across your product
Phase three puts the full governance model in place and scales agentic AI across the product. With one or two workflows proven, you standardize the audit trail, the decision boundaries, and the review process, then extend them to new workflows instead of reinventing controls each time. This is where agentic AI tools become a real capability across the product.
On build, buy, or integrate: own your governance and audit infrastructure, since it is core to a healthcare product. Scale deliberately, with controls that satisfy auditors, and you can add new workflows without reopening the same compliance questions every time.
Our Experience Building Agentic AI for Healthcare Products
At TechMagic, we have built AI-powered features for healthcare products. In every one, the product decisions mattered more than the model, and they decided whether the feature shipped. Across our HealthTech work, we have shipped agentic and AI-driven workflows for clinical documentation, prior authorization, patient intake, and decision support, always with steady care delivery as the goal.
Technically, the pattern repeats. We ground each agent in real clinical context with Retrieval Augmented Generation over Fast Healthcare Interoperability Resources (FHIR) data and the unstructured notes around it. We minimize and tokenize protected health information at each step, log an auditable decision trail, and run the workflow on a HIPAA-aligned, mostly serverless AWS stack.
None of the hard parts are surprises. The big one is integrating agentic AI with messy clinical data: you map records into FHIR and merge them with the free-text notes before an agent can reason over the full picture. The rest is scope and trust, so you keep the feature narrow enough to stay clear of Software as a Medical Device (SaMD) rules, and you earn the confidence of the clinicians who sign off.
Tiro.Health: making clinical data capture usable
On the Tiro.Health medical form platform, the blocker was adoption, because clinicians abandon a tool that fights them. We built the frontend around clean, FHIR-mapped data capture and met Web Content Accessibility Guidelines (WCAG) 2.2, so the product works for every user. The result is a form layer clinicians actually complete, which is what makes any automation underneath it worth shipping.
MHC Healthcare: compliance built into the architecture
On the MHC Healthcare EHR portal, patient privacy and data security set the architecture from day one. We designed the data model, role-based access, and an end-to-end audit trail before feature work began, instead of bolting compliance on at review. The result is a HIPAA-compliant build where every action on patient data is traceable, which is the exact foundation an agentic feature needs.
Unumed: securing a cloud-native system before it ships
Our security background shapes how we treat agentic workflows, and TechMagic holds CREST accreditation alongside SOC 2 and ISO 27001 compliance services. On Unumed's cloud-native hospital management system, our penetration test probed the same multi-step, multi-service surface that an agent expands. We surfaced and helped close vulnerabilities before they reached production, which is why we treat data security as a design input from the first sprint.
What carries across the work
The decisions that separate success are consistent. Close the context gap first, scope narrowly, design governance early, and build the audit trail from day one. These are product decisions, and they are where we spend our time.
The main points of focus are the data, the scope, and the checkpoints around the model.
Check our:

Final Thoughts
The pilot era in healthcare AI is ending, and the bar keeps rising. Gartner expects 33% of enterprise software applications to include agentic AI by 2028, up from less than 1% in 2024. The teams that get there win on product decisions made early: a closed context gap, a narrow scope, governance designed before it is needed, testing against clinical edge cases, and an audit trail built from day one.
Where is this heading?
Context becomes the moat. The agents that reach production will be the ones wired into complete clinical data, while polished demos on a fraction of the record keep stalling.
Governance moves to the front. Oversight is turning into a build requirement, so the teams that design decision boundaries and audit trails early will ship while others wait on compliance reviews.
Regulation catches up to autonomy. The FDA has already authorized more than 1,400 AI-enabled medical devices, and as agents start to influence clinical decisions, SaMD lines will be tested far more often. The products that scoped autonomy deliberately will adapt fastest.
Agentic systems run on structure. Multi-agent systems in a clinical product depend on defined boundaries and a clear audit trail to operate safely at scale.
The teams treating these as product decisions now will be best positioned when the tooling matures.

FAQ

Most healthcare AI pilots fail to reach production because of product and architecture decisions made before any agent code is written; the model is rarely the cause. The three recurring reasons are incomplete context, undefined scope, and absent governance.
Agentic AI for medical products differs from general enterprise AI because of four healthcare-specific constraints: Software as a Medical Device (SaMD) classification risk, protected health information (PHI) exposure across multi-step workflows, electronic health records (EHR) integration complexity, and liability when an agent acts autonomously. These constraints shape where you place human checkpoints and what the audit trail must hold.
An agentic AI feature in a healthcare product can require FDA clearance once it influences a clinical decision rather than only handling administrative work. An agent that recommends a diagnosis or suggests a treatment plan may qualify as Software as a Medical Device (SaMD); an agent that only drafts documentation usually does not. Confirm the classification with a regulatory opinion before you build.
To scope an agentic AI workflow for a medical product, we start with one high-value workflow at lower clinical risk, such as documentation, prior authorization, or patient intake. We define what the agent may and may not do, put a clinician in the loop for high-risk steps, and add a rollback path. We expand only after that first workflow is stable in production.
A production-ready agentic AI audit trail in healthcare records every decision: the input context, the action taken, the tools called, the human approval status, and the outcome, each with a timestamp and with raw PHI kept out of plain text. This audit trail is the evidence auditors and regulators ask for, so build it from day one.
The time to move from a healthcare AI pilot to production depends on the workflow's clinical risk, your data readiness, and your governance maturity, so a credible estimate comes only after scoping. Teams that close the context gap and scope one workflow narrowly tend to move faster than teams that try to automate everything at once.
Yes, we have built AI-driven and agentic workflows for HealthTech products, including clinical documentation, prior authorization, patient intake, and decision support, under HIPAA and other compliance constraints. TechMagic's work spans EMR portals, medical form platforms, and security testing of healthcare systems.